


 Filed Under: Health Economics | Health Plans
Filed Under: Health Economics | Health Plans

Three Ways H.R. 1 will Drive Transformative Changes in Medicaid
When Congress passed H.R. 1, better known as the “One Big Beautiful Bill” it generated an array of conversations around the future of Medicaid. Written into the legislation were major provisions that would have sweeping implications for Medicaid directors, statewide policymakers, enrollees, providers, and health plans.
Over the course of the spring, ProgenyHealth has met with and heard from healthcare leaders and policymakers from around the country on the future of Medicaid. At the center of nearly every conversation was the impact of H.R. 1. In this blog, we will focus on three key areas of concern for stakeholders: eligibility, technology, and funding.
Eligibility

H.R. 1’s eligibility framework is designed to reduce Medicaid enrollment, with an end goal of promoting greater workforce participation. However, policy experts warn that documenting compliance with work requirements could be particularly difficult for gig workers, farmers, and seasonal employees who struggle to document hours worked. Lessons from the Medicaid unwinding post-COVID, are shaping current strategies, with some MCOs preparing to take an active role in outreach and communication in partnership with states. Still unresolved are critical issues such as the definition of “medical frailty,” and ex parte eligibility, both of which will significantly affect who retains coverage under H.R. 1.
Technology
H.R. 1 is driving substantial technology investment. However, many stakeholders at the state level claim they do not have sufficient time to build new systems before the January 1, 2027 deadline and will instead rely on modifying existing technology platforms. Many of these platforms lack basic data-sharing capabilities, making interoperability a central challenge. Real-time data exchange will become essential and is expected to be required in the second year of H.R. 1. Unlike the COVID-era unwinding, federal funding may not cover implementation costs, potentially leaving states to absorb significant upfront expenses. While some technology funding may eventually become available, there is a concern it will not arrive in time to support initial compliance, forcing states to modernize while simultaneously implementing policy.
Funding
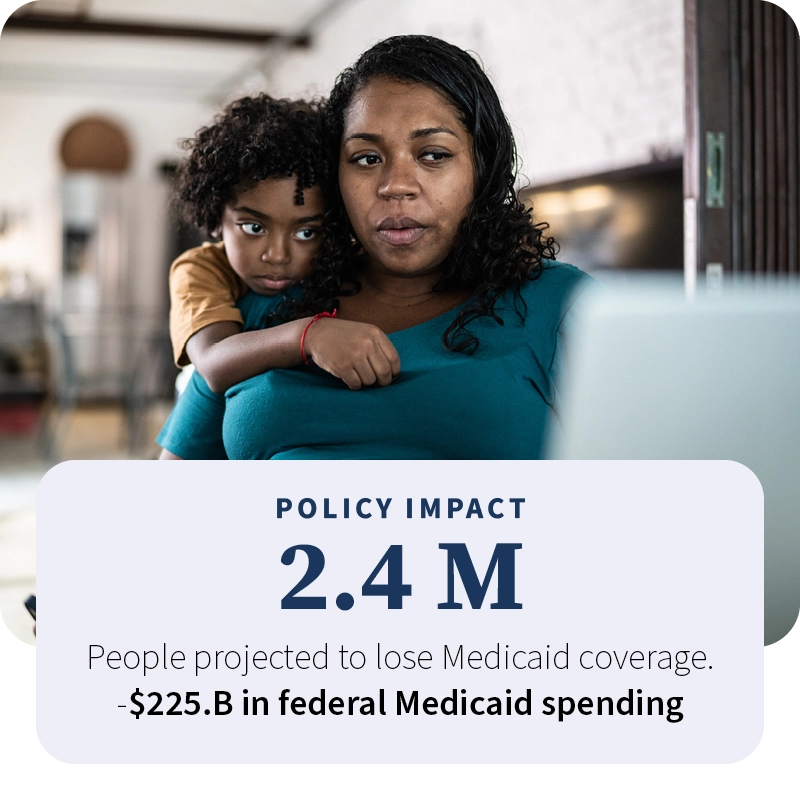
Perhaps the most profound impact of H.R. 1 is financial: dollars are shifting away from delivering care and toward administering eligibility, work requirements, and compliance. At the same time, the federal government is transferring more Medicaid and SNAP costs to states while restricting traditional revenue tools such as provider taxes and state-directed payments. When funding tightens, states are left with limited options—cut provider rates, reduce benefits like adult dental, or narrow eligibility for certain populations. The downstream effects could be significant: rising uncompensated care, financial strain on hospitals, and broader economic consequences as coverage losses ripple through local economies. Without new, flexible financing mechanisms, H.R. 1 risks recreating a pre-ACA environment marked by instability for providers, states, and beneficiaries alike.
Strategy Matters
As the provisions of H.R. 1 begin to be felt, it is crucial that stakeholders collaborate to proactively plan for and address the associated challenges. By anticipating the scale and scope of these policies, more can be done to tamper their potentially challenging downstream effects. Working to address savings levers, clinical collaboration, and improving overall outcomes, via specialized partners is just one way to address the uncertainty.
 Prev
PrevView All Posts
Stay Informed
Subscribe to the latest maternity + NICU updates & news